Lower back pain is one of the most common and most misunderstood health complaints worldwide. Stuart McGill, distinguished professor emeritus at the University of Waterloo and chief scientific officer at Backfitpro, has dedicated his career to unraveling its complexities. His work offers both scientific clarity and real-world hope to patients who have struggled for years without relief.
The Anatomy of Pain
McGill begins with fundamentals: the structure of the spine and how the lower back functions under stress. He explains that the spine is not a single moving part but a system of joints, muscles, and connective tissues that interact dynamically. Weakness or instability in any of these areas can set the stage for injury.
Challenging “Nonspecific Back Pain”
A central theme in McGill’s approach is his rejection of the label “nonspecific back pain.” Rather than accept pain without explanation, he emphasizes the importance of finding the causal link between an injury and its symptoms. According to McGill, clarity is not just possible—it’s essential for recovery.
Lessons from Complex Cases
Through case studies, McGill demonstrates how careful assessment and targeted treatment have resolved severe, long-standing pain. These stories show that with the right strategy, even patients who have been told there is “nothing more to do” can regain their mobility and quality of life.
Building Strength and Stability
Beyond diagnosis, McGill stresses prevention and resilience. His core message: strength and stability protect the spine. He shares his go-to exercises designed to reinforce spinal health and help patients move with less pain. These exercises aren’t about heavy lifting—they’re about building control, endurance, and protective strength.
Practical Advice for a Healthy Spine
McGill’s guidance goes beyond the clinic. He offers everyday strategies to keep the back strong: mindful movement, proper lifting techniques, and maintaining a balance between activity and rest. His conviction is simple yet powerful: nobody needs to suffer endlessly from back pain.
Outline
0:00:30 – Peter’s experience with debilitating back pain 0:14:11 – Anatomy of the back: spine, discs, facet joints, and common pain points 0:24:48 – Lower back injuries and pain: acute vs. chronic, impact of disc damage, microfractures, and more 0:31:30 – Why the majority of back injuries happen around the L4, L5, and S1 joints 0:37:20 – How the spine responds to forces like bending and loading, and how it adapts do different athletic activities 0:45:12 – The pathology of bulging discs 0:48:33 – The pathophysiology of Peter’s back pain, injuries from excessive loading, immune response to back injuries, muscle relaxers, and more 0:59:36 – The three most important exercises Stuart prescribes, how he assesses patients, and the importance of tailored exercises based on individual needs and body types 1:12:46-The significance of strength and stability in preventing injuries and preserving longevity 1:25:33-Stuart’s take on squats and deadlifting: potential risks, alternatives, and importance of correct movement patterns 1:37:08-Helping patients with psychological trauma from lower back pain by empowering them with the understanding of the mechanical aspects of their pain 1:46:59-Empowering patients through education and understanding of their pain through Stuart’s clinic and work through BackFitPro 1:56:08-When surgical interventions may be appropriate, and “virtual surgery” as an alternative 2:05:48-Weakness, nerve pain, and stenosis: treatments, surgical considerations, and more 2:11:21-Tarlov cysts: treatment and surgical considerations 2:13:34-The evolution of patient assessments and the limitations of MRI 2:18:40-Pain relief related to stiffness and muscle bulk through training 2:26:49-Advice for the young person on how to keep a healthy spine 2:39:24-Resources for individuals dealing with lower back pain
Today we will explore the evolving landscape of dementia, with a particular focus on Alzheimer’s disease, Lewy Body dementia, and Frontotemporal dementia. Whether you are a clinician, caregiver, researcher, or someone navigating these conditions with a loved one, this episode aims to inform and empower.
We begin with the etiology of Alzheimer’s disease, a condition whose origins are multifactorial. The disease arises from a complex interplay of genetic predispositions, environmental exposures, and lifestyle factors. At the cellular level, the accumulation of amyloid-beta plaques and tau neurofibrillary tangles disrupts neuronal communication, triggers inflammatory responses, and ultimately results in widespread synaptic dysfunction and neuronal loss.
Additional contributors include chronic neuroinflammation, oxidative stress, and mitochondrial dysfunction. Genetically, while early-onset familial Alzheimer’s is rare and linked to a variety of mutations, the APOE ε4 allele remains the strongest risk factor for late-onset Alzheimer’s. Vascular pathology, sleep disturbances, diabetes, and poor cardiovascular health also play critical roles in disease onset and progression.
Lets consider the classification of dementia types. Alzheimer’s disease remains the most prevalent, accounting for approximately 60 to 70 percent of cases. Other types include vascular dementia, Lewy Body dementia, Frontotemporal dementia (FTD), mixed dementias, and less common conditions such as Creutzfeldt-Jakob disease and normal pressure hydrocephalus.
Frontotemporal dementia frequently presents between the ages of 45 and 65 and manifests with profound changes in personality, language, or behavior. It is commonly divided into three subtypes: behavioral variant FTD, primary progressive aphasia, and FTD with motor neuron disease or ALS. Familial inheritance is seen in a substantial number of cases.
In contrast, Lewy Body dementia typically affects individuals over the age of 65 and is characterized by fluctuating cognition, recurrent visual hallucinations, REM sleep behavior disorder, and parkinsonian motor features. These patients often exhibit severe sensitivity to antipsychotic medications, necessitating careful pharmacologic management.
In terms of diagnostics, the field is rapidly advancing. Biomarkers derived from cerebrospinal fluid, such as decreased Aβ42 and elevated phosphorylated tau, along with PET imaging for amyloid and tau pathology, now allow for earlier and more accurate diagnosis. Recently, FDA-approved blood-based tests like Lumipulse are improving access to non-invasive diagnostic tools. The A/T/N biomarker framework further enables clinicians to classify patients by underlying pathology rather than clinical symptoms alone.
Treatment options remain limited in terms of disease modification, but several monoclonal antibodies have demonstrated promise. Lecanemab and donanemab, for example, have shown statistically significant slowing of cognitive decline in early-stage Alzheimer’s patients. However, risks such as amyloid-related imaging abnormalities (ARIA) must be carefully managed. Ongoing trials are investigating additional compounds, including amyloid vaccines and anti-inflammatory therapies.
Living with dementia requires more than pharmacology, it demands a comprehensive care model. The GUIDE Program, a Medicare initiative launched in 2024, offers care navigation, caregiver support, and community-based resources. The program’s aim is to reduce caregiver burden, delay institutionalization, and improve quality of life through a structured, coordinated approach.
Finally, for those seeking support, numerous resources are available. These include memory care clinics, the Alzheimer’s Association’s 24/7 helpline, adult day centers, caregiver education, and long-term care planning services. Technology, such as wearable devices and smart home tools, can also enhance safety and independence.
This concludes today’s episode. For further information, please refer to the show notes for links to GUIDE, the Swank Memory Center, and biomarker updates. Thank you for listening and as always, we encourage you to stay informed and proactive in the pursuit of brain health.
Detailed Outline
ETIOLOGY
The etiology of Alzheimer’s disease (AD) is multifactorial and involves a complex interplay of genetic, environmental, and lifestyle factors.
🧠 Core Pathological Mechanisms
1. Amyloid-β Plaques
Accumulation of misfolded Aβ42 peptides leads to extracellular plaques.
These disrupt cell signaling, trigger inflammation, and may initiate synaptic dysfunction.
2. Tau Neurofibrillary Tangles
Hyperphosphorylated tau proteins aggregate inside neurons.
They impair microtubule transport and contribute to cell death.
3. Neuroinflammation
Chronic activation of microglia and astrocytes leads to neurotoxicity.
Alzheimer’s likely results from a convergence of amyloid and tau pathology, neuroinflammation, genetic vulnerability, and lifestyle/environmental risk factors. Current research focuses on early biomarkers, disease-modifying interventions, and prevention strategies targeting modifiable risks.
TYPES
🧠 1. Alzheimer’s Disease (AD)
Most common type (~60–70%)
Caused by accumulation of amyloid-β plaques and tau tangles.
Key features: Memory loss, disorientation, language difficulties, impaired judgment.
Progression: Gradual and irreversible; begins with short-term memory impairment.
🧠 2. Vascular Dementia
Second most common; caused by reduced blood flow to the brain due to strokes or microvascular disease.
Potentially reversible with ventriculoperitoneal shunting.
🧠 8. Creutzfeldt-Jakob Disease (CJD)
Rapidly progressive, caused by prion proteins.
Key features: Myoclonus, ataxia, severe cognitive decline.
Prognosis: Typically fatal within months.
🧠 9. Other Rare Causes
Huntington’s disease
Chronic traumatic encephalopathy (CTE)
HIV-associated dementia
Autoimmune/paraneoplastic limbic encephalitis
Toxic/metabolic (e.g., alcohol-related)
Frontotemporal Dementia (FTD) is a group of neurodegenerative disorders primarily affecting the frontal and temporal lobes of the brain. It typically presents earlier than other dementias, often between ages 45 and 65, and is the second most common cause of dementia in people under 65.
🧠 Subtypes of FTD
1. Behavioral Variant FTD (bvFTD)
Most common type.
Symptoms:
Apathy, disinhibition, loss of empathy, socially inappropriate behavior
Poor judgment, impulsivity
Changes in eating habits or compulsive behaviors
Often mistaken for psychiatric illness (e.g., depression or bipolar disorder).
2. Primary Progressive Aphasia (PPA)
Language-dominant presentation, with two main subtypes:
Nonfluent/agrammatic variant (nfvPPA):
Halting, effortful speech
Impaired grammar and sentence construction
Semantic variant (svPPA):
Fluent but empty speech
Loss of word meaning and object recognition
3. FTD with Motor Neuron Disease (e.g., ALS)
Overlap of FTD symptoms with signs of motor neuron degeneration.
Rapid progression and poorer prognosis.
🧬 Causes and Genetics
30–40% of cases are familial with known gene mutations:
MAPT (tau)
GRN (progranulin)
C9orf72 repeat expansion (also seen in ALS)
Pathology may involve tau, TDP-43, or FUS protein accumulation, depending on subtype.
🔍 Diagnosis
Clinical assessment focused on personality, behavior, and language changes.
Cognitive testing: May appear normal in early disease despite major functional impairment.
💊 Treatment
No cure or FDA-approved disease-modifying therapies.
Management is symptomatic:
SSRIs or trazodone for disinhibition or compulsive behavior.
Speech therapy for PPA.
Support for caregivers due to challenging behavioral symptoms.
Cholinesterase inhibitors (e.g., donepezil) used in Alzheimer’s typically not helpful and may worsen symptoms.
📉 Prognosis
Progressive and ultimately fatal.
Average survival: 6–11 years after symptom onset.
Faster progression with motor involvement.
Lewy Body Dementia (LBD) is a progressive neurodegenerative disorder characterized by the abnormal accumulation of alpha-synuclein protein (Lewy bodies) in the brain. It’s the second most common cause of dementia after Alzheimer’s disease, accounting for 10–15% of cases.
🧠 Key Clinical Features
1. Fluctuating Cognition
Marked variations in attention, alertness, and executive function.
Patients may appear lucid at times and profoundly confused at others.
2. Visual Hallucinations
Recurrent, well-formed, and detailed (e.g., people, animals).
Often occur early in the disease course.
3. Parkinsonism
Bradykinesia, rigidity, postural instability, and sometimes tremor.
May resemble idiopathic Parkinson’s disease, but typically follows or coincides with cognitive decline.
4. REM Sleep Behavior Disorder (RBD)
Acting out dreams during REM sleep.
Often precedes other symptoms by years.
5. Autonomic Dysfunction
Orthostatic hypotension, constipation, urinary incontinence, and temperature dysregulation.
6. Neuroleptic Sensitivity
Severe worsening of symptoms or life-threatening reactions to typical antipsychotics (e.g., haloperidol).
🧪 Diagnosis
Clinical criteria: Based on presence of core and suggestive features.
FTD: Usually absent early (except in FTD-ALS variant)
LBD: Parkinsonian features common and early
🧠 Hallucinations/Delusions
FTD: Rare
LBD: Common, especially visual hallucinations early in disease
🧠 Cognitive Fluctuations
FTD: Stable progression
LBD: Day-to-day or hour-to-hour variation in alertness and cognition
🧠 Response to Medications
FTD: May worsen with cholinesterase inhibitors
LBD: Cholinesterase inhibitors can help cognition and hallucinations
Extreme sensitivity to antipsychotics (may cause severe worsening)
🔬 Pathology
FTD: Tau, TDP-43, or FUS protein inclusions
LBD: Lewy bodies (alpha-synuclein aggregates)
🧬 Genetics
FTD: 30–40% familial; known mutations (MAPT, GRN, C9orf72)
LBD: Rarely familial; most cases sporadic
🧪 Imaging
FTD: Frontal and/or temporal lobe atrophy
LBD: Occipital hypometabolism on PET; relative sparing of hippocampus
📉 Prognosis
FTD: 6–11 years from symptom onset
LBD: ~5–8 years from diagnosis
DIAGNOSIS
🧠 Early Diagnosis: Faster, Less Invasive, More Accurate
1. Core CSF Biomarkers
These reflect the hallmark pathologies of Alzheimer’s disease:
Amyloid-beta 42 (Aβ42): Decreased levels in CSF indicate amyloid plaque deposition in the brain.
Total tau (t-tau): Increased levels reflect neuronal damage and degeneration.
Phosphorylated tau (p-tau, especially p-tau181 or p-tau217): Elevated levels correlate with tau tangles and are more specific to AD than total tau.
2. PET Imaging Biomarkers
Used to visualize pathology in vivo:
Amyloid PET (e.g., using florbetapir, florbetaben, or flutemetamol): Detects fibrillar amyloid plaques.
Tau PET (e.g., using flortaucipir): Detects paired helical filament tau deposits.
FDG-PET: Shows hypometabolism in the temporoparietal cortex, typical of AD.
3. MRI Biomarkers
Structural imaging to assess brain atrophy:
Medial temporal lobe atrophy, especially in the hippocampus, is characteristic.
Cortical thinning in the parietal and posterior cingulate regions can also be supportive.
4. Emerging Blood-Based 🩸 Biomarkers
More accessible and scalable than CSF or PET (LabCorp, Quest, Hospital)
Plasma Aβ42/Aβ40 ratio: Lower ratios may indicate amyloid pathology.
Plasma p-tau217: Show strong correlation with AD pathology.
FDA-approved blood test for amyloid detection
In May 2025, the FDA cleared the blood-based test
Fujirebio’s Lumipulse (pTau217, β‑Amyloid ratio)
5. Genetic Biomarkers
Used for risk assessment, especially in early-onset or familial cases:
APOE ε4 allele: Strongly associated with increased AD risk but not diagnostic.
Mutations in APP, PSEN1, PSEN2: Rare, associated with early-onset familial AD.
Biomarker Framework
The A/T/N classification is now used to describe biomarker status:
A: Amyloid (CSF Aβ42 or amyloid PET)
T: Tau (CSF p-tau or tau PET)
N: Neurodegeneration (CSF t-tau, FDG-PET, or structural MRI)
This framework helps stratify individuals by their underlying biology regardless of symptoms.
💊 Therapeutics: New and Emerging Options
Monoclonal antibodies targeting amyloid
1. Lecanemab (Leqembi)
•A large Phase III trial (Clarity AD) involving 1,795 participants with early Alzheimer’s disease showed a 27% slowing in clinical decline over 18 months versus placebo, with significant amyloid reduction verified by PET.
2. Donanemab (Kisunla)
•The TRAILBLAZER-ALZ 2 Phase III trial (1,736 individuals) reported a ~35% slower progression over 76 weeks based on composite scales (iADRS, CDR‑SB).
•Particularly, individuals with mild cognitive impairment experienced up to 60% slower decline on iADRS.
•Gained FDA accelerated approval in 2021, but its clinical benefit remains controversial due to inconclusive trial results and high adverse-event rates.
4. Next‑Generation Candidates
•Trontinemab (Roche) demonstrated rapid amyloid reduction—with 81% of patients reaching sub-24 Centiloid levels in just 28 weeks of Phase II data.
•Gantenerumab, though halted in general populations, showed benefit in genetically at-risk individuals in a 2025 study.
•TB006, targeting galectin‑3, recently showed promising Phase II results and ongoing Expanded Access in the US.
Clinical Significance & Caveats
•Meta-analyses confirm mAb therapies robustly clear amyloid and slow decline—but the clinical impact is moderate, and benefit may be questionable for late-stage or rapidly progressed cases.
•Adverse events, particularly ARIA (brain swelling/hemorrhage), occur in 15–40% of patients depending on agent and dosage.
Repurposed cancer drugs show promise
– A UCSF study found cancer drugs letrozole + irinotecan significantly reversed symptoms in Alzheimer’s mouse models.
– Analysis of patient records suggests lower Alzheimer’s prevalence among users, paving the way for clinical trials.
Pipeline developments
– Over 180 clinical trials are ongoing, exploring over 130 novel compounds targeting amyloid, tau, inflammation, and synaptic health.
– Investigational approaches include amyloid vaccines, secretase inhibitors, tau aggregation blockers, and saracatinib (a synaptic enhancer).
Innovative delivery methods
– Breakthrough research includes brain-implanted graphene devices and nasal vaccines aiming for targeted neural stimulation.
🌱 Symptom Management & Prevention
Cholinesterase inhibitors & memantine
– Standard treatments—donepezil, rivastigmine, galantamine, and memantine—continue to offer modest symptomatic relief; don’t halt neurodegeneration.
Lifestyle interventions
– Emphasis on heart-healthy habits: regular exercise, Mediterranean/MIND diet.
– Nutritional supplements, e.g. omega‑3, B‑vitamins, evidence mixed.
RESOURCES
🏥 Medical & Clinical Support
Neurology clinics – for diagnosis, medication management, and care planning.
Memory care centers – multidisciplinary teams focused on cognitive disorders.
Geriatric psychiatry – for behavioral symptoms like anxiety, agitation, or hallucinations.
Home health agencies – provide nursing, therapy, personal care services in the home.
🧭 Caregiver & Patient Education
Alzheimer’s Association (www.alz.org)
24/7 helpline: 1-800-272-3900
Dementia Friendly America (www.dfamerica.org)
National Institute on Aging (www.nia.nih.gov)
🤝 Support Groups & Counseling
In-person/virtual support groups for patients and caregivers.
Individual/family counseling – licensed therapists who specialize in aging.
Adult day centers – supervised environments for socialization, activities, respite.
🏡 Residential & Long-Term Care Options
In-home care aides – for activities of daily living (ADLs).
Assisted living with memory care units – secure environments with trained staff.
Skilled nursing facilities – for more advanced needs and medical support.
Hospice and palliative care – for late-stage support focused on comfort.
📄 Legal and Financial Planning
Elder law attorneys, for power of attorney, guardianship, wills, and Medicaid planning.
Financial planners, to manage long-term care funding, insurance, and asset protection.
Social workers/case managers – connect families with available benefits and programs.
🧘♀️ Technology & Daily Living Aids
GPS trackers, cameras (WYZE), Apple Watch, medical alert devices.
Medication reminders, automatic dispensers
Smart home tools – for lighting, appliances, and emergency response.
Memory aids – whiteboards, calendars, visual cues, labeled drawers.
💰 Financial Assistance
Medicare/Medicaid
Veterans Administration (VA) Aid & Attendance
State aging agencies and Area Agencies on Aging (www.n4a.org)
Long-term care insurance, if previously purchased.
GUIDE Program
The GUIDE Model (Guiding an Improved Dementia Experience) is an eight-year, voluntary Medicare initiative launched July 1, 2024, by the Centers for Medicare & Medicaid Services (CMS). It aims to enhance dementia care quality and support for patients and their unpaid caregivers through structured, coordinated services.
🧩 Core Components
1. Care Navigation: Each person with dementia and their caregiver is paired with a Care Navigator who provides ongoing support, care coordination, and access to community services and respite care.
2. Nine Required Service Domains: Includes comprehensive assessments (e.g., Clinical Dementia Rating), individualized care planning, 24/7 helpline access, regular monitoring, medication reviews, caregiver education, coordination with services, respite support, and specialist referrals.
3. Caregiver Education & Respite: Caregivers are provided training and structured respite services (e.g., adult day centers) to alleviate burden and delay institutionalization.
4. Alternative Payment Model: Instead of fee-for-service, participating providers receive a per-beneficiary monthly dementia care management payment (DCMP), adjusted for complexity, geography, caregiver presence, and performance.
🎯 Goals & Benefits
1. Keep patients at home longer and reduce unnecessary hospital or long-term care admissions.
2. Reduce caregiver strain via education, support, and respite resources.
3. Address social determinants of health by screening and connecting families to community resources.
4. Improve health equity, prioritizing underserved populations with performance-linked incentives.
🏥 Participation & Eligibility
Eligible providers: Medicare Part B-enrolled clinicians and health systems.
Two tracks:
Established programs start July 2024.
New programs go live July 2025 after a planning period.
Eligible beneficiaries:
Medicare Part A/B (non-Medicare Advantage),
Diagnosed with dementia (any stage),
Living in the community (not in nursing homes or hospice) .
The Health app now allows you to set up a Sleep Schedule that works with your Sleep Focus on iPhone to help you get a good night’s sleep. Find out how to set up Sleep in the Health app.
Go to bed on time with a bedtime reminder on your iPhone.
Get a healthy amount of sleep by setting up a Sleep Schedule and Sleep Goal on your iPhone.
How to Set Up Sleep in the Health App
System Requirements
This tip was performed on an iPhone 16 running iOS 18.3.1. Find out how to update to the latest version of iOS.
You can use the Sleep in the Health app to improve your sleep routine. Here’s how to use Sleep to set up Sleep Goals on your iPhone, change Sleep Goals, set up a Sleep Schedule, set a Bedtime Reminder and wakeup alarm, and more. Now, here’s how to set up Sleep in the Health app:
Open the Health app.
Tap the Browse tab.
Scroll down and tap Sleep.
If this is your first time accessing the Sleep settings, tap Get Started to set up your Sleep Schedule.
Tap You do not have a Sleep schedule under Full Schedule & Options.
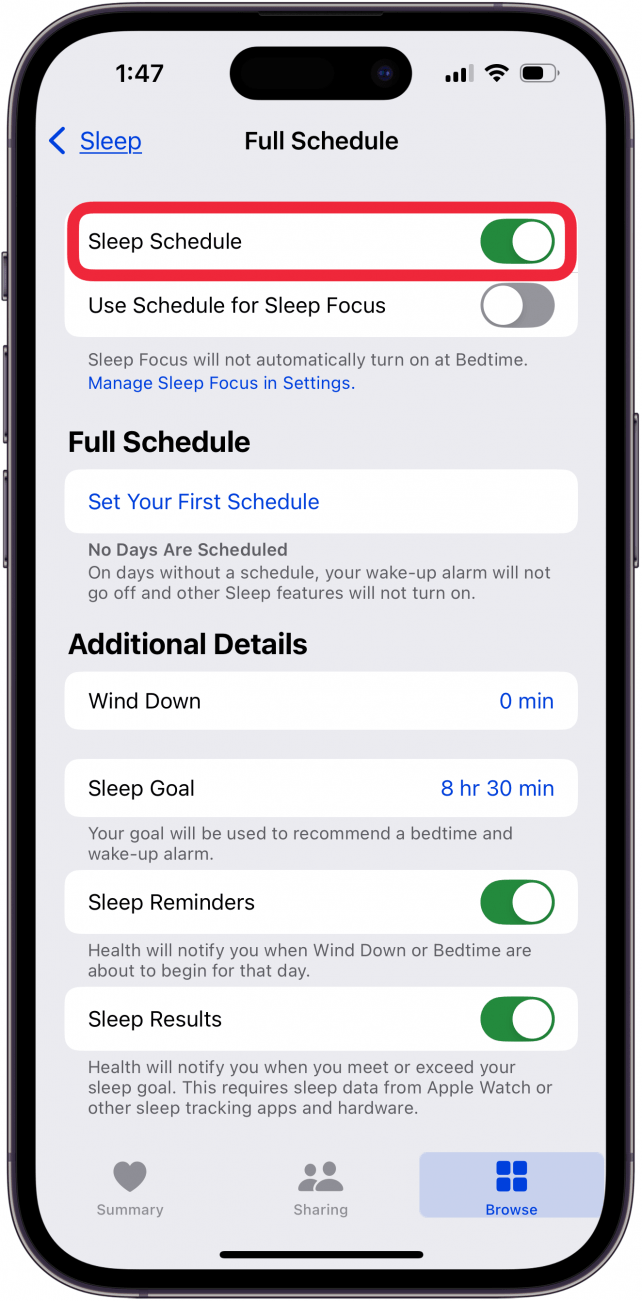
Toggle on Sleep Schedule.
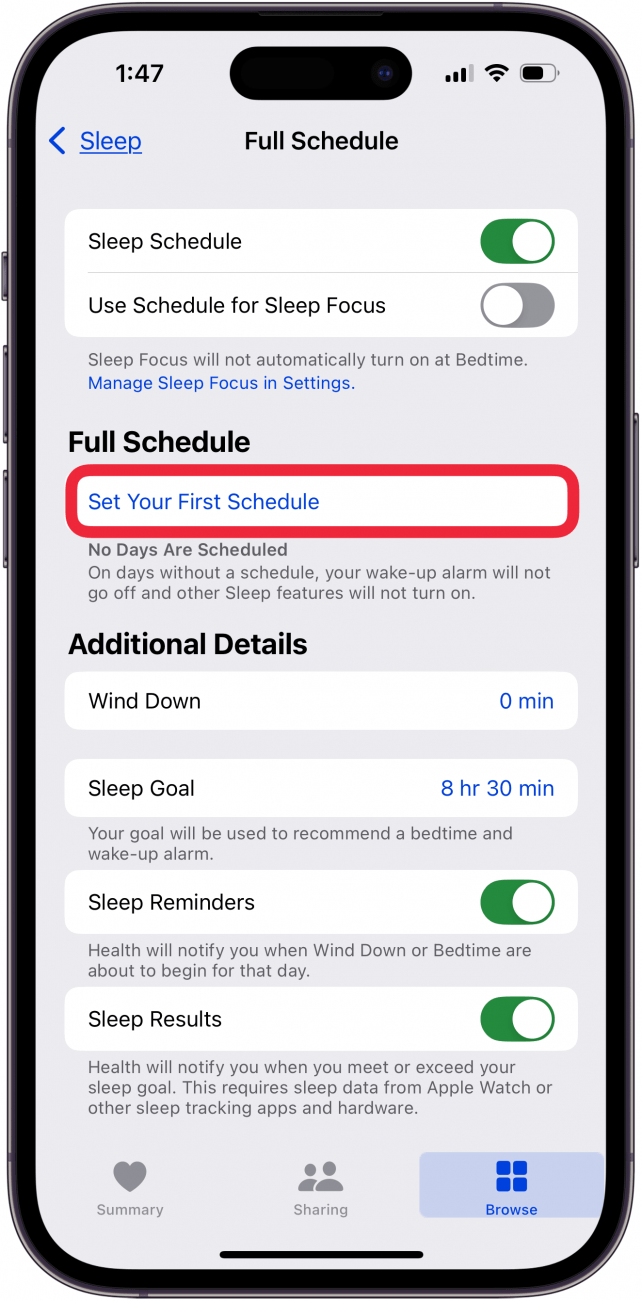
Tap Set Your First Schedule.
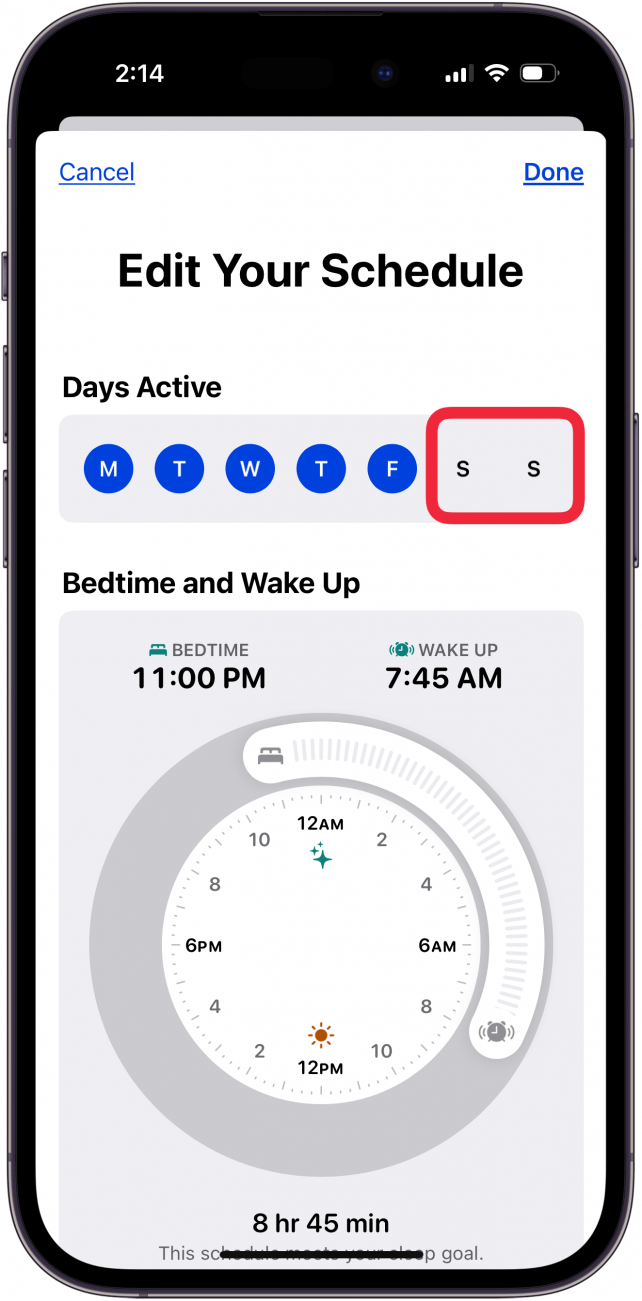
Tap the days you DON’T WANT included in your sleep schedule.
To set your bedtime and wake-up times, drag the Bedtime and Wakeup sliders to when you want to go to sleep and wake up.
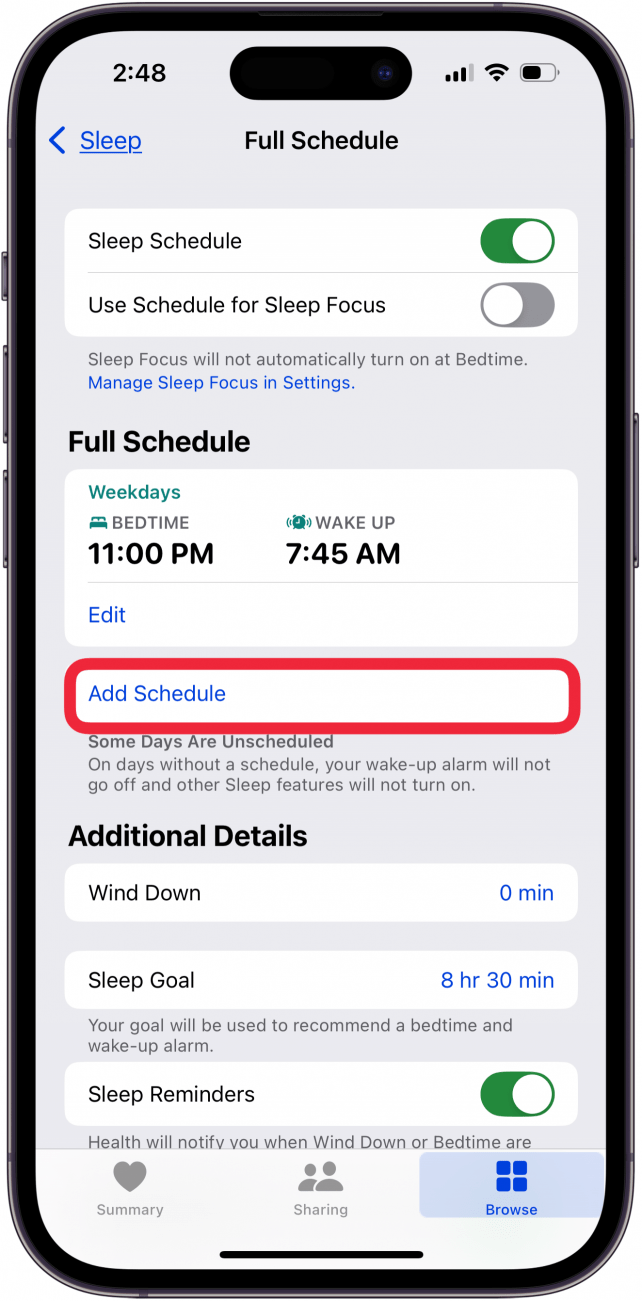
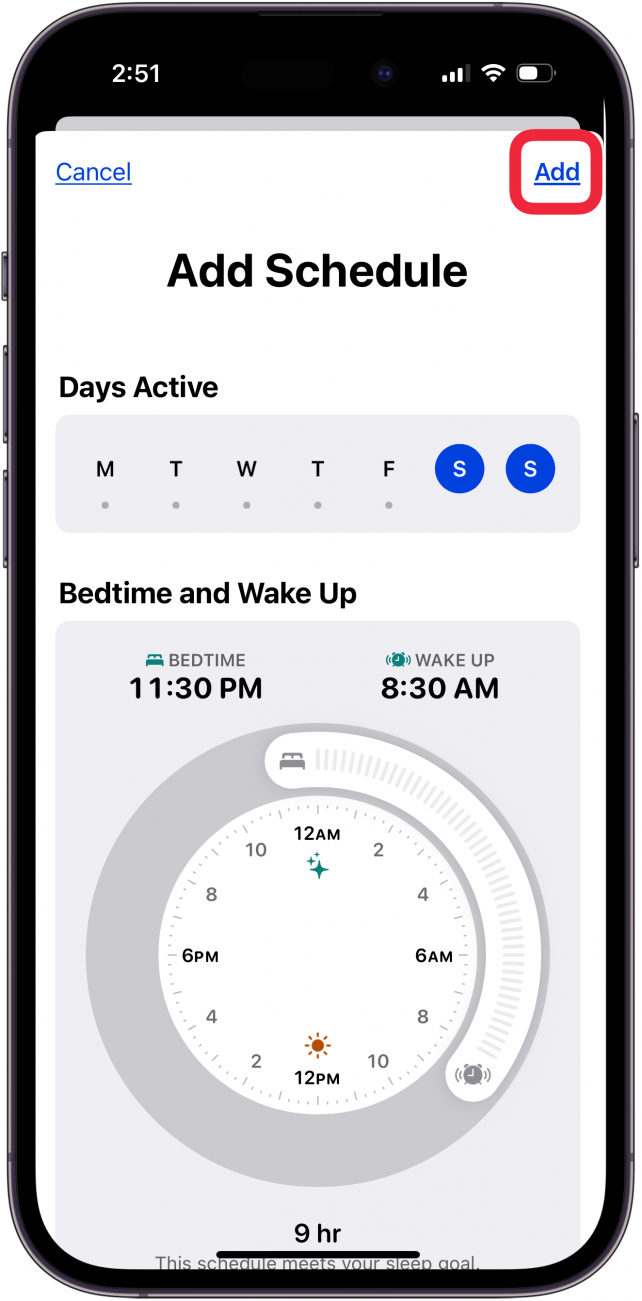
If you have multiple sleep schedules, you can tap Add Schedule.
The unscheduled days (in this case Saturday and Sunday) will be highlighted, and you can use the Bedtime and Wakeup sliders to set the sleep schedule as before, and tap Add.
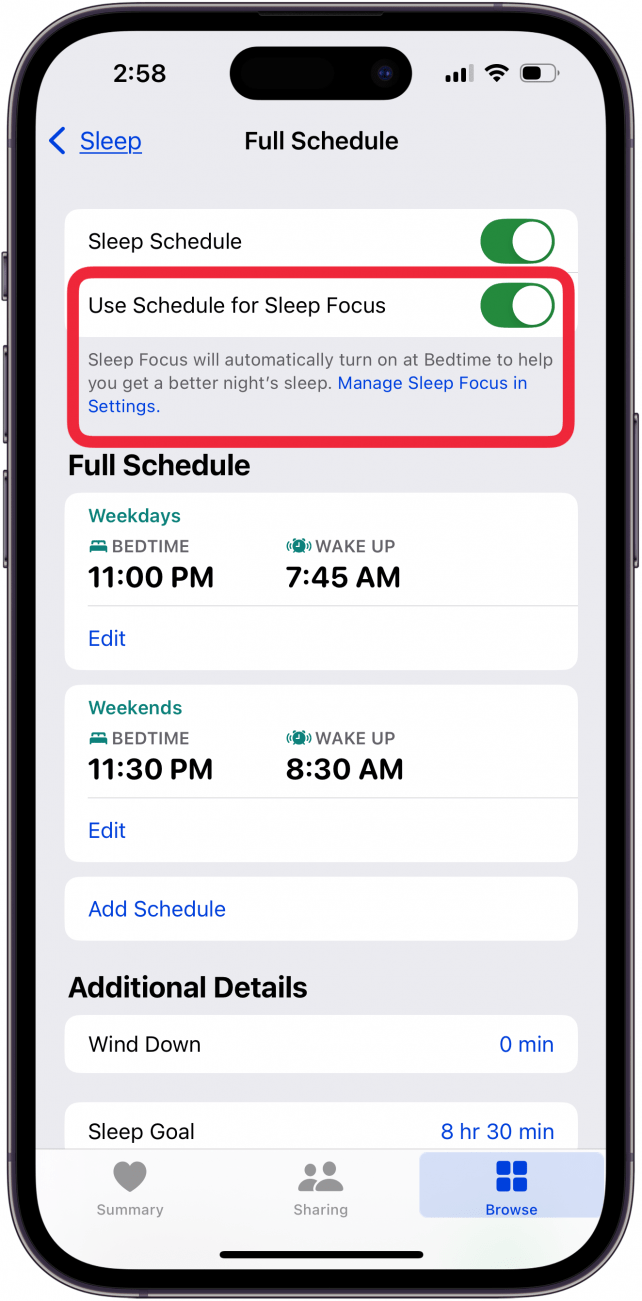
Toggle on Use Schedule for Sleep Focus to have your Sleep Focus turn on automatically at Bedtime. If this is your first time setting up Sleep, this menu may look different than the screenshot below.
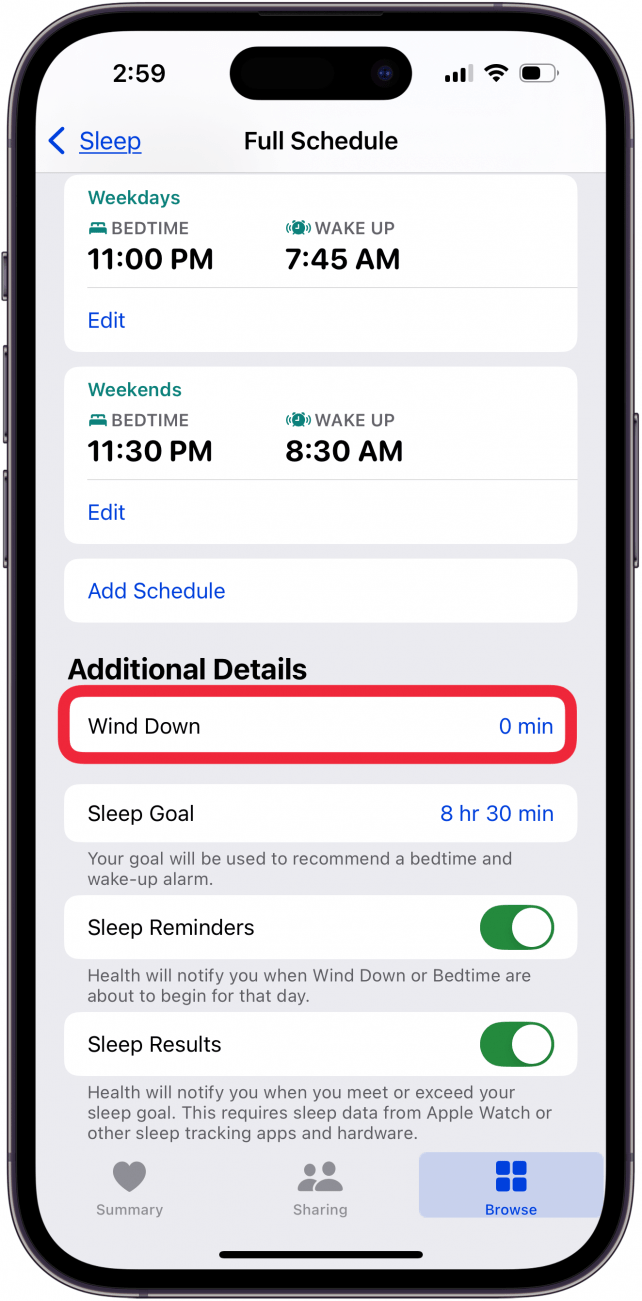
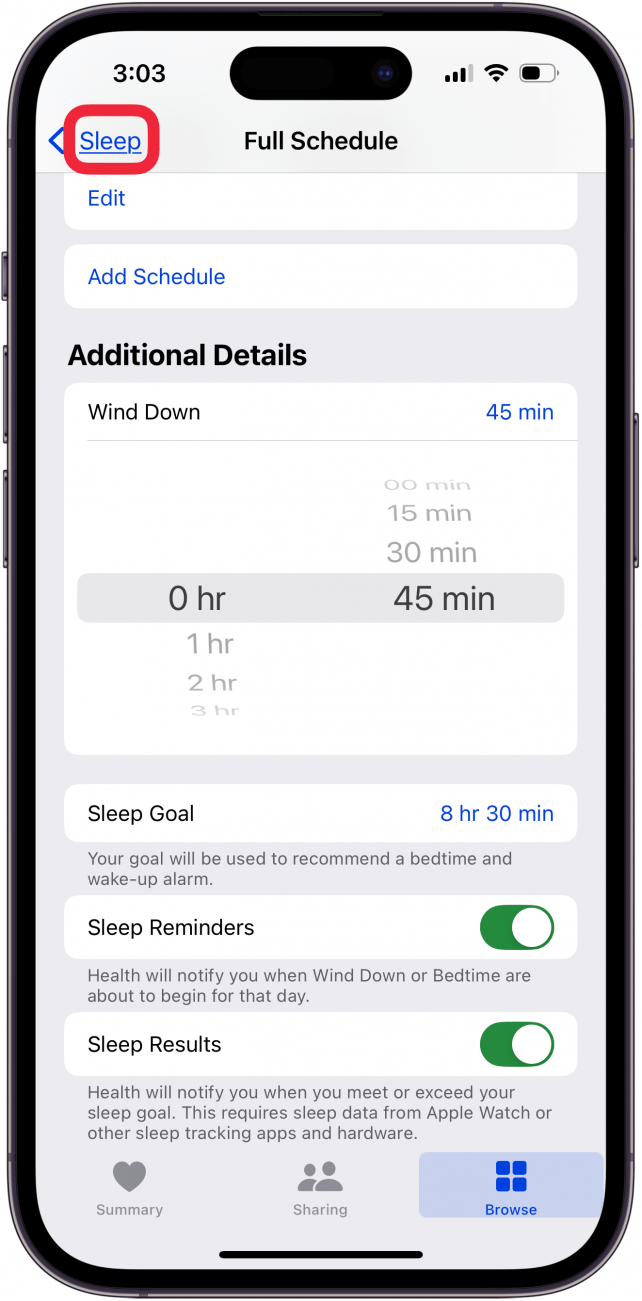
Tap Wind Down under Additional Details.
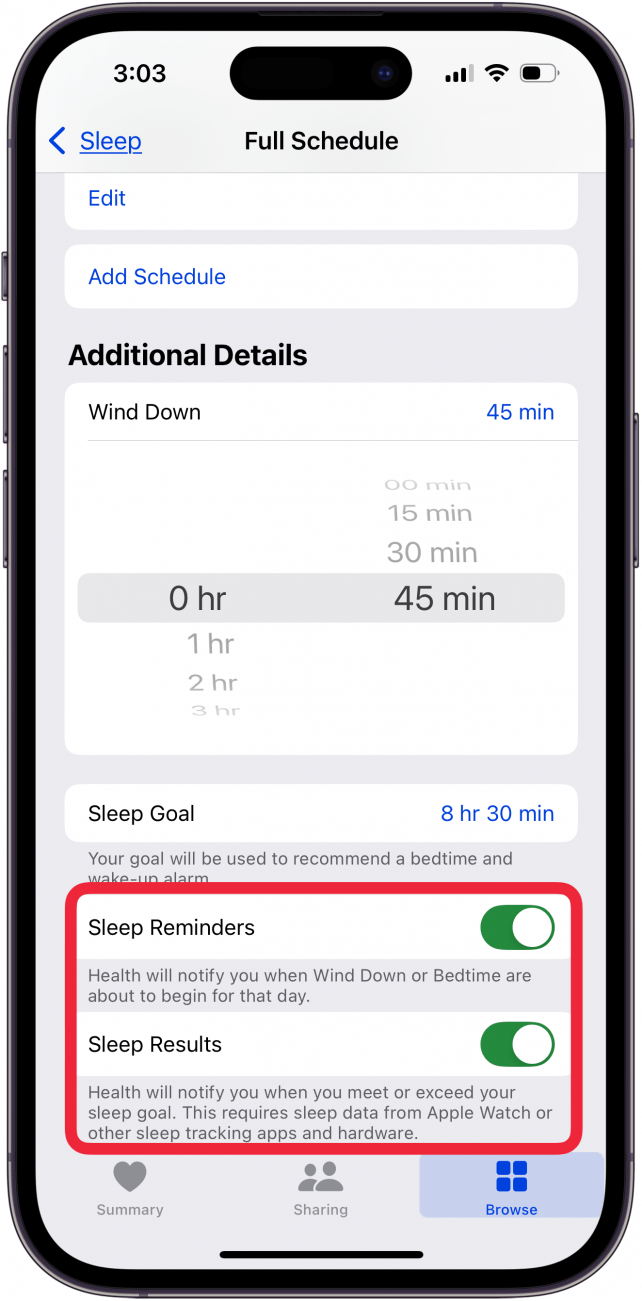
Scroll to set how long before bed you would like to start winding down. If this is your first time setting a Wind Down time, this menu may look different than the screenshot below.
You can also toggle on Sleep Reminders and Sleep Results.
Tap Sleep to return to the previous page.
If you ever want to edit your Sleep Schedule, simply repeat steps 1-3, and then scroll down and find Your Schedule. Then, tap Edit under Next to only edit your next Sleep Schedule.
Tap Full Schedule & Options to edit your full schedule, as well as adjust settings like Wind Down time and your Sleep Goal.
Now you’ve set up Sleep in the Health app! You can adjust your schedule whenever you want, and if you have an Apple Watch, you can see data like respiratory rate, heart rate, and how many hours of sleep you are averaging.
A recent important study published in Nature Medicine examines the impact of long-term adherence to various dietary patterns on healthy aging.
Utilizing data from the Nurses’ Health Study and the Health Professionals Follow-Up Study – over 100K people in their early fifties followed for 30 years – in the end, only 23% of them were free of 11 chronic diseases!
Primary Message: Eat well and believe the science.
Study Parameters
Healthy Aging Better Cognitive Function Better Physical Function Better Mental Health Free from Chronic Disease Survival Past Age 70
Key Findings:
Dietary Patterns: Higher adherence to healthful dietary patterns, such as the Alternative Healthy Eating Index (AHEI), was associated with increased odds of healthy aging. Participants in the highest quintile of AHEI adherence had an 86% greater likelihood of aging healthily compared to those in the lowest quintile.
Beneficial Foods: Increased consumption of fruits, vegetables, whole grains, unsaturated fats, nuts, legumes, and low-fat dairy products correlated with better aging outcomes.
Not surprisingly, healthy options include vegetables, fruits, unsaturated fats, nuts, legumes, omegas-3s and fish. And surprisingly (you’ll like this!), wine, fast food, fried food for better chances of brain health & longer life!
Detrimental Foods: Higher intakes of trans fats, sodium, sugary beverages, and red or processed meats were inversely associated with healthy aging.
Unhealthy food, as expected, included trans fats, total meats, red meat, butter, margarine, snacks, sodium, processed meats, sweets and desserts, sugary juices, total alcohol and refined grains. Surprisingly, potatoes & starchy vegetables, low energy drinks were net negatives
A Deep Dive into Cognitive Behavioral Therapy for Insomnia
Summary of a podcast by Dr Peter Attia and Ashley Mason
Introduction
Ashley Mason, PhD, is an Associate Professor at UCSF, leading the Sleep, Eating, and Affect (SEA) Lab and directing the COAST Center. Her work focuses on non-pharmacologic treatments for mood, sleep, and eating disorders, with a central focus on cognitive behavioral therapy for insomnia (CBT-I). In a conversation that serves as a master class, Dr. Mason breaks down the science, structure, and strategies of CBT-I—an intervention she champions as life-changing and highly effective.
• Eliminate sleep medications gradually with precision and physician support.
• Avoid rotating OTC and prescription meds—standardize and stabilize.
CBT-I Implementation at UCSF
• Program Structure: Intake → 5 weekly group sessions → follow-up.
• Group Format: 8 patients per cohort; group dynamic enhances adherence.
• Telemedicine: Fully remote access for California patients.
The Role of Digital Tools and AI
• Current apps show moderate promise, but personalization and accountability are challenges.
• Dr. Mason supports the development of AI-assisted programs (e.g., Rest) to democratize CBT-I.
Additional Sleep Disruptors to Rule Out
• Sleep Apnea / RLS: Screen and refer before starting CBT-I.
• Medication Side Effects: Some blood pressure meds suppress melatonin.
Practical Behavioral Advice
• Avoid Napping: Unless >80 years old, limit to 25 minutes max.
• Middle-of-the-Night Awakenings: Leave bed, do boring (non-stimulating) tasks until sleepy again.
• Social Jet Lag: Never sleep in two days in a row; choose which weekend day to feel rested.
Sleep, Anxiety, and the Cognitive Link
• Track belief in distressing thoughts across the day—most lose power by afternoon.
• CBT-I reframes distorted sleep-related beliefs, improving both sleep and mood.
Thermal Interventions and Future Research
• Sauna: May help some; trial shows promise combining heat therapy + CBT-I.
• Cold Plunge: Discouraged before bed—raises core temp post-exposure.
Takeaway
“You don’t have to know what caused your insomnia. Just do the treatment. It works when you do it.” – Dr. Ashley Mason
CBT-I is among the most effective psychological treatments available, with 70% of patients achieving clinically meaningful results. While adherence is essential, the payoff is substantial—better sleep, improved functioning, and often, life transformation. No one should have to suffer from insomnia. Access may be challenging, but tools exist—from books to digital apps—that can initiate recovery.
A few days ago, the Delaware Health and Human Development Committee held a critical hearing on end-of-life legislation. The discussion was robust, focusing on essential issues such as patient autonomy, the unfounded fears of a ‘slippery slope,’ the role of hospice care, and the perspectives of physicians and advanced practice nurses. The time has come for Delaware to affirm its commitment to compassionate, patient-centered care by enacting medical aid in dying (MAID) legislation.
Patient Choice is Paramount
MAID is fundamentally about the right of individuals to make deeply personal decisions about their own bodies and lives. It does not impose any obligation on patients or physicians who choose not to participate, making it a model of respect for diverse values. The era of medical paternalism is over. We now recognize that patients—armed with medical guidance and personal convictions—are best suited to determine their own end-of-life care. Denying them this choice is not a safeguard; it is an infringement on their autonomy and dignity.
The Myth of the ‘Slippery Slope’
Opponents of MAID frequently cite the so-called ‘slippery slope,’ warning that legalizing medical aid in dying will lead to unchecked expansion and abuse. Yet, decades of data from the 11 states where MAID is legal provide no evidence to support these claims.
Medical ethicist Thaddeus Pope points out that the combined experience with MAID in these states spans over a century. The laws, largely modeled after Oregon’s Death with Dignity Act, have been in place since 1997, operating with strong safeguards and oversight. If there were any validity to the ‘slippery slope’ argument, we would have seen clear evidence by now. Instead, what we have is a proven framework that ensures patient choice while maintaining rigorous protections. Rather than succumbing to fear-based hypotheticals, Delaware should move forward with evidence-based legislation that reflects the real-world experience of other states.
Hospice Care and MAID Go Hand-in-Hand
Some argue that MAID is an alternative to quality end-of-life care, but the reality is quite the opposite. Data from Oregon, Washington, and California consistently show that more than 90% of patients who request MAID are already enrolled in hospice care. MAID is not about replacing palliative care; it is about giving terminally ill patients one more option in their final days. It provides peace of mind to those who, despite receiving the best hospice services, wish to exert control over their suffering.
Physician Support Reflects a Changing Medical Ethos
The medical community overwhelmingly supports MAID. Surveys consistently show that up to 70% of physicians favor giving patients this option. A recent Delaware physician survey mirrored national trends, demonstrating widespread professional support. Physicians—who bear witness to the suffering of their patients daily—understand the profound relief MAID can offer. It is time for policymakers to listen to those on the front lines of healthcare and align legislation with the evolving medical consensus.
Delaware’s Second Chance to Do the Right Thing
In 2024, the Delaware legislature approved end-of-life legislation, only to see it vetoed by the governor. This year, lawmakers have another opportunity to stand on the right side of history by reaffirming their support for patient autonomy and compassion. Passing House Bill 140 would grant the people of Delaware the fundamental right to make informed, personal decisions about their own healthcare.
This is not a partisan issue—it is a human one. It is about dignity, respect, and the recognition that every individual should have the right to determine how they meet life’s final chapter. The evidence is clear, the safeguards are strong, and the need is undeniable. The Delaware legislature must act now to pass MAID legislation and ensure that patients facing unbearable suffering have the freedom to make the choice that is right for them.
“Excess adiposity should be confirmed by at least one other anthropometric criterion (eg, waist circumference) or by direct fat measurement when available. However, in people with substantially high BMI levels (ie, >40 kg/m2) excess adiposity can be pragmatically assumed
People with confirmed obesity (that is, with clinically documented excess adiposity) should then be assessed for possible clinical obesity based on findings from medical history, physical examination, and standard laboratory tests…”
Track sleep, heart rate, respiratory rate, temperature, blood oxygen, and sleep duration on your Apple Watch. Here’s how, from iPhone Insider (Dr Bob recommends signing up for lots of great tips and guidance on how to use your Apple Watch and iPhone 🤗
In the latest version of watchOS, the Apple Watch now has a dedicated Vitals app. The Vitals app collects your health data as you sleep and brings it all together in one convenient location. Let’s take a look at the new Apple Watch Vitals app.
Keep track of your health data in one convenient app.
Compare your current vitals with the previous week.
How To Use the Vitals App on Apple Watch
System Requirements
This tip works on Apple Watches running watchOS 11 or later. Find out how to update to the latest version of watchOS.
One of the best Apple Watch features is the ability to track your sleeping habits, like your average respiratory rate and heart rate. Now, the Vitals app provides you with a breakdown of your heart rate, respiratory rate, wrist temperature, blood oxygen level, and your sleep duration. All of this data is available in one convenient app. Here’s how to navigate the Vitals app on Apple Watch:
Open the Vitals app.
If this is your first time opening this app, you’ll be greeted by an explanation of the app. Scroll down and tap Next.
You’ll also be asked to enable notifications for this app. Tap Enable or Skip.
At the top, you’ll see an overall look at your Overnight Vitals. Tap the info icon for more details on what your vitals mean.
You can scroll down and select More Info.
This screen will tell you the difference between Typical and Outlier vitals. Tap the X to close this screen.
Scroll down to see individual breakdowns of each of your vitals. First, is Heart Rate. Like the Overnight Vitals, you can tap the info icon for more details on each Vital.
Scroll down to see your Respiratory Rate.
Next, is your Wrist Temperature.
Continue scrolling to see your Blood Oxygen level.
Lastly, you can see your Sleep Duration, which is how much sleep you got the night before.
You can tap the Calendar icon to toggle between Today’s Vitals and the past 7 days’ Vitals.
This will show you how your vitals last night compare to the previous 7 days.
That’s how to navigate the new Vitals app in watchOS 11. Each of these data points can be found in separate apps, like Heart Rate, Blood Oxygen, and Sleep, so it’s nice to have it all available at a quick glance. The Vitals app will learn you typical sleep behaviors and if there is ever an outlying bit of data, you’ll get a notification to help you improve your sleep.
Which foods should we point the finger at? Due to their saturated fat content, foods such as tropical oils (palm or coconut oil), baked goods, sweets and foods that have been fried all contribute to an increase of ‘bad’ cholesterol.
Processed meats – think sausages, bacon and hot dogs – also contain a high amount of saturated fat. According to one review involving 614,000 participants, each additional 50g (1.8oz) serving of processed meat per day is linked to a 42 per cent higher chance of heart disease.
Then there’s sugar. It also acts like a drug on your liver, encouraging it to produce more LDLs and fewer HDLs. A 15-year study found that participants who took in 25 per cent or more of their daily calories in sugar were more than twice as likely to die from heart disease, with cholesterol playing a key role.
I suddenly wore two hats — that of a retired physician who had cared for people with Alzheimer’s disease and now a person living with the same disorder.
I have a special interest in Alzheimer’s disease. For nearly 25 years, I practiced general neurology in Portland, Oregon, and some of my patients had dementia. In 2012, while doing a genealogical DNA search, I inadvertently discovered that I have two copies of the APOE-4 allele, meaning I had a very good chance of getting Alzheimer’s-caused dementia by age 80. I felt gobsmacked. I remember walking down the stairs in a daze after reading the report from the genetic testing service and telling my wife, Lois, “I think I am screwed.”
A year later, I retired at age 62 even though I had no symptoms of cognitive impairment. If I had almost any other job, I could have continued working for a few more years, but in medicine, forgetfulness could have fatal consequences. I suddenly wore two hats — that of a retired physician who had cared for a lot of people with Alzheimer’s disease and now a person living with the same disorder.
I had been taught, in medical school in the 1970s and even during my neurology residency in the 1980s, that Alzheimer’s disease progresses from onset to death in about three to five years, and nothing can be done about it. Neither statement is true.
In hindsight, my first symptom of Alzheimer’s disease was a gradual loss of smell that I first noticed in 2006. This was accompanied by odd olfactory hallucinations that smelled like baking bread mixed with perfume. I didn’t have any measurable cognitive impairment until 2015, when I had significant trouble remembering words, including the names of friends and colleagues.
I had a PET scan as part of a research study, which showed my brain had the beginning of abnormal tau protein, a key part of diagnosing Alzheimer’s. When the scans were repeated in 2018 and 2022, the tau protein can be seen spreading through my brain.
We now know that the first signs of Alzheimer’s disease, beta-amyloid plaques, can be seen in the brain up to 20 years before any cognitive changes. Tau-containing tangles start to form later, about two or three years before the onset of mild cognitive impairment. There is a variation in the speed of progression from mild impairment to full-blown dementia to death, probably about eight to 12 years on average.
I am now 73, and I have had mild cognitive impairment for roughly five years, followed by mild dementia for about four years. We don’t yet have a way to stop this progression, but what have I been doing to slow it?
There are lifestyle modifications that help, and they also decrease the likelihood of getting it in the first place.
Top among them is aerobic exercise. Multiple studies have shown up to a 50 percent reduction in the chance of getting Alzheimer’s disease for people who exercise regularly. The only group that doesn’t seem to benefit from exercise are those who already have dementia. The sooner you start, the better.
I started exercising daily in 2012 as soon as I learned that I was on the Alzheimer’s trajectory. Recent evidence shows that tai chi can help people who already are experiencing cognitive impairment.
The data for adopting a plant-based diet are almost as strong as exercise. I follow a variant of the Mediterranean diet called the MIND diet that includes eating foods with increased flavonols such as nuts and certain vegetables. Many experts now recommend avoiding alcohol, especially for people with a family history of dementia. Recently, I gave up my daily glass of beer or wine. Frankly, I have been surprised that nonalcoholic beer tastes quite good.
Staying mentally active is very important. For me, my most important brain exercise is reading and writing. I do a crossword puzzle every day while eating lunch, and I enhance the brain benefit by looking up words I don’t know. Staying socially engaged is important but increasingly difficult as dementia progresses. It’s best for me to socialize with just one or two people at a time. Getting at least 7½ hours of sleep each night appears to reduce the chance of getting dementia.
What about drugs? We now have two FDA-approved drugs, lecanemab and donanemab, that are effective in removing beta-amyloid from the brain, but they only slow cognitive decline by about 35 percent. They can also have lethal side effects in patients with two copies of the APOE-4 allele, like me. After only four monthly injections of aducanumab (a cousin of lecanemab) during the phase 3 trial, I developed swelling and bleeding in my brain requiring a stay in an intensive care unit and about four months to recover. The drug has since been discontinued by its manufacturer.
These treatments represent an important step forward in understanding the neurobiology of Alzheimer’s disease, but they should not be used by everyone.
So I have learned that Alzheimer’s disease is not the rapidly progressive dementia I was taught about in medical school. It is a slowly progressive disease that is asymptomatic for up to 20 years. Mild symptoms of cognitive impairment may be annoying but usually can allow normal activities for another five years or so. Even work may be possible with accommodations. Once someone has dementia, unable to live independently, lifestyle modifications and medications do not seem to be as effective. In my experience, it is critical to manage Alzheimer’s disease in the early stages to postpone the onset of dementia. Don’t wait for the horses to get out of the barn.