Your favorite beverage may be doing serious damage to your health.
Sugar-sweetened beverages may increase your risk for heart disease and type 2 diabetes, new research finds.
Sugary drinks were found to be linked to over 330,000 deaths a year.
A study published in Nature Medicine analyzed global data on sugar-sweetened beverages (SSBs) consumed around the world from both observational and randomized studies, as well as diabetes and cardiovascular disease prevalence.
On a global level, researchers found that 2.2 million new cases of type 2 diabetes and 1.2 million new cases of heart disease in 2020 were attributable to SSBs—representing about 1 in 10 new type 2 diabetes cases and 1 in 30 new heart disease cases.
“For the past century, heart disease has remained the leading cause of death in the United States. Fortunately, as our understanding of the disease has evolved over time, we have made advances in treatment options to help people reduce their risk for a devastating cardiovascular event, like a heart attack or stroke.
But staying one step ahead of this disease requires both providers and patients to continually follow and implement the latest science and regulatory guidance on what treatment options are safe, effective, and FDA-approved. Sadly, this isn’t happening and misinformation about treatment options poses a significant public health concern, which the FDA has acknowledged and in July issued new guidance on how companies can combat it.”
A new study reveals that the prevalence of atherosclerosis is alarmingly high among asymptomatic adults classified as “low risk” and underscores the importance of lipid-lowering therapies for avoiding atherosclerosis progression and mortality
Recently, the CDC’s National Center for Health Statistics released its preliminary report on mortality data from 2023. Once again, heart disease reigned supreme as the leading cause of death in the United States1 – a sorry distinction it has held firmly for the last two decades.
Heart disease – and more specifically, coronary atherosclerosis, which is responsible for the majority of deaths from cardiovascular disease – is easily the most preventable of all the “four horsemen of chronic disease” (i.e., heart disease, cancer, neurodegenerative disease, and metabolic disease). It is causedby apoB-containing lipoproteins (90-95% of which are low-density lipoproteins, or LDLs), which penetrate artery walls and initiate atherogenesis. Thus, therapies for lowering circulating LDL levels – such as statins, PCSK9 inhibitors, and others – have the power to virtually stop atherosclerosis in its tracks. So why does this disease remain a top killer? A study published last month provides some insights, along with further evidence of the importance of lowering LDL as a means of preventing atherosclerosis-related mortality.2
About the study
Study authors Faridi et al. analyzed data from the Miami Heart Study, which involved participants who were 40-65 years of age and free of any clinically evident cardiovascular disease (CVD) at enrollment.3 From this cohort, the present study excluded any participants with additional risk factors for atherosclerosis, including hypertension (systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg), diabetes, or tobacco use, as well as any individuals who were taking lipid-lowering medications. This left Faridi et al. with a final cohort of 1,033 participants (median age of 51 years at the time of enrollment; 55% women) with no CVD symptoms and at relatively low risk based on the exclusion criteria.
As part of the original Miami Heart Study, participants had undergone cardiac imaging tests at baseline, including coronary artery calcification (CAC) scans and contrast-enhanced coronary computed tomography angiography (CCTA) scans. Laboratory tests were also performed to assess baseline blood lipids. In the present study, Faridi et al. utilized these cross-sectional baseline data to determine the prevalence of coronary atherosclerosis among low-risk, asymptomatic adults, as well as to characterize its associations with atherogenic lipoprotein concentrations as estimated by LDL cholesterol (LDL-C) or non-HDL-cholesterol (non-HDL-C), or directly measured by apoB levels.
A high prevalence of atherosclerosis in low-risk adults
Despite their evident “low risk” status, over one third (35.9%) of participants included in the analysis were found to have coronary plaque, while roughly one quarter (25.3%) had a CAC score over zero – an indication of the presence of early-stage artery calcification. Additionally, a smaller set of participants were found to have more advanced CVD, with 4.5% having CAC scores ≥100 (indicating moderate disease), 3.4% showing evidence of high-risk plaque, and 1.9% demonstrating artery blockage of at least 50% according to CCTA scans.
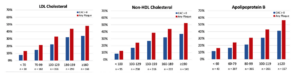
The proportion of participants with coronary plaque increased with increasing serum levels of LDL-C, non-HDL-C, and apoB (see Figure below). Specifically, after adjusting for covariates, each 10 mg/dL increase in LDL-C was associated with a 13% increase in risk (OR: 1.13; 95% CI: 1.08-1.18), each 10 mg/dL increase in non-HDL-C was associated with a 12% increase in risk (OR: 1.12; 95% CI: 1.08-1.16), and each 10 mg/dL increase in apoB was associated with a 20% increase in risk (OR: 1.20; 95% CI: 1.13-1.27). The somewhat stronger association between plaque and apoB compared to associations with LDL-C or non-HDL-C is in line with expectations, as atherogenesis depends on the number of apoB-containing lipoproteins (as indicated by apoB levels) rather than on their cholesterol content (as indicated by LDL-C or non-HDL-C). Importantly, the increases in risk with increasing lipoprotein levels appeared to be linear down to at least 70 mg/dL LDL-C – well below the American Heart Association’s current guideline of <100 mg/dL as an “optimal” value.4 Across lipoprotein strata, risk was also observed to increase with age and was higher among men than among women, which agrees with earlier reports on sex differences in atherosclerosis progression and adverse cardiovascular events.5
Figure: Prevalence of coronary atherosclerosis among low-risk adults based on serum lipid and lipoprotein concentrations. Prevalence of coronary atherosclerosis (as detected by CCTA) and coronary artery calcium (as detected by CAC scan) is shown as a percentage of participants within each stratum of lipoprotein levels. Cholesterol values are in mg/dL. Adapted from Faridi et al. 2024.²
The authors also performed analyses on a subgroup consisting of the very lowest-risk participants, defined by more stringent risk factor thresholds than the full cohort (e.g., systolic blood pressure <120 mm Hg, diastolic blood pressure <80 mm Hg, BMI <25 kg/m2). Within this subgroup (n=184; 83.7% women), prevalence of coronary plaque was lower than in the full cohort but still alarmingly common, as it was observed in 21.2% of these “optimal risk” participants. CAC scores above zero were reported for 14.7% of the subgroup, though none of these participants demonstrated CAC scores ≥100 or ≥50% artery blockage.
A silent but avoidable killer
In all, Faridi et al.’s results reveal a startlingly high prevalence of early- to moderate-stage coronary atherosclerosis among patients classified as “low risk” with no reported symptoms such as chest pain or shortness of breath. Further, they show that higher levels of apoB-containing lipoproteins were associated with higher risk, even when comparing levels below those regarded as optimal by current guidelines. While this was an observational study based on cross-sectional data and on its own tells us nothing about any causal relationship between apoB and cardiovascular disease, these results align with a large, consistent body of evidence indicating that apoB-containing lipoproteins drive the development of atherosclerosis – and that reducing serum levels of apoB-containing lipoproteins, for instance with statins or PCSK9 inhibitors, can slow or halt the progression of this disease and help to prevent subsequent major adverse cardiovascular events such as heart attacks or strokes.
Thus, we return to the question posed at the start of this piece – why is atherosclerotic cardiovascular disease so deadly despite the existence of effective treatments? The results of the present study suggest a simple (albeit alarming) answer: millions of individuals with this disease are likely unaware of it. Atherosclerosis develops over decades of exposure to high levels of circulating apoB-containing lipoproteins, yet for those who are relatively young or otherwise healthy, both patients and physicians often ignore the possibility of coronary artery disease, failing to test for it via CAC or CCTA scans even when LDL-C is known to be elevated.
Faridi et al.’s data show that apparent health is no guarantee of the absence of CVD, and as we’ve seen in a previous newsletter, being proactive about lipid and imaging tests – and following up with appropriate treatments – can literally be the difference between life and death. On a population scale, these actions have the power to put an end to mortality from coronary atherosclerosis. One horseman down, three to go.