So, critically, none of these human studies tell us anything about how fluoride changes the brain at a biological level. Even studies in lab animals and cells did not identify how fluoride might affect learning, memory, or intelligence.
IQ scores also only capture an incomplete picture of early childhood brain development and are tangled up in a number of socioeconomic, racial, and culturalfactors beyond how much fluoride someone is exposed to.
If you’re concerned about your family’s fluoride exposure, you can check your tap water’s fluoride levels on the CDC’s My Water’s Fluoride page. If you happen to live somewhere with levels above around 1.5 mg/L, your tap water crosses the threshold of neurodevelopmental concern. No need to switch to bottled water, though; home water purifiers can filter fluoride out completely.
To make sure you don’t throw out the oral health benefits of fluoride with the bathwater, keep using fluoride toothpaste for those over the age of 2 (just don’t swallow it).
And if you’re still fluoride-skeptical, you can order some hydroxyapatite toothpaste— which has similar cavity-preventive benefits — from Europe or Canada, where it’s been approved and endorsed by dental associations.
1. Eli Lilly is now selling single-dose vials of Zepbound for about half of its usual monthly list price through its direct-to-consumer platform LillyDirect. The drugmaker is offering a four-week supply of 2.5-milligram vials for $399 and 5-milligram single-dose vials for $549. In comparison, the list prices for GLP-1 weight loss drugs are typically about $1,000 a month.
2. Novo Nordisk CEO Lars Fruergaard Jørgensen defended the cost of Wegovy this week, arguing it will lower obesity care costs for patients and employers, NBC Nightly News reported Aug. 25. Last year, obesity care costs totalled more than $400 billion. Mr. Jørgensen told the outlet that employers and patients may see lower medical costs, disability payments, workers’ compensation and absenteeism as people lose weight on the medications. He also noted that more than 80% of insured Americans pay $25 or less for a month’s supply.
3. Recent studies have highlighted significant economic and racial disparities in access to GLP-1 weight loss drugs, The Washington Post reported Aug. 19. Lower-income and Black and Hispanic populations have higher rates of obesity and Type 2 diabetes but face significant barriers due to high costs and limited insurance coverage, according to the report.
4. GLP-1s may reduce mortality and severe cardiovascular complications in patients with obesity, according to a study published Aug. 22 in Diabetes, Obesity and Metabolism.
5. GLP-1s may also help improve medication adherence rates among heart patients, Jeffrey Wessler, MD, a cardiologist at New Hyde Park, N.Y.-based Northwell Health, toldBecker’s.
“In my view, and I think where the evidence is bringing us, is that what started as a medication for diabetics and weight loss is quickly becoming probably one of the best cardiac medications that exists,” he said. “That’s for a fairly simple reason, which is that it may be the first medication that patients actually want to take because it has this amazing side effect of losing weight.”
6. Some physicians are growing more comfortable prescribing compounded versions of Wegovy and Zepbound amid shortages of the brand-name versions, according to anecdotal reports shared with NBC News. Though the FDA permits licensed compounding pharmacies to produce medications during shortages, some physicians remain skeptical, citing concerns that the agency does not regulate or test the active ingredients used by these pharmacies.
Eli Lilly announced that it would start selling low doses of its weight-loss drug Zepbound in vials, too — at a far lower price than its pens, which come with pre-filled doses. These vials will be made available only through LillyDirect, a telehealth platform the company launched in January that connects patients with providers who can prescribe obesity drugs. Like compounded drugs prescribed by online startups, Zepbound vials can be delivered right to patients’ doors.
Insurance hurdles and worries about muscle loss mean fewer older patients are using weight-loss drugs
Millions of people are flocking to drugs like Ozempic and Wegovy to lose weight and treat health problems. Doctors say one group that could benefit from the drugs is missing out: seniors.
For older people, these medications can help in ways that go beyond losing weight, physicians say. Fewer pounds can lead to more mobility and better balance, allowing older people to become more active. That can boost mood, overall health, and sometimes makes the difference between walking freely or using a wheelchair or cane.
A new study reveals that the prevalence of atherosclerosis is alarmingly high among asymptomatic adults classified as “low risk” and underscores the importance of lipid-lowering therapies for avoiding atherosclerosis progression and mortality
Recently, the CDC’s National Center for Health Statistics released its preliminary report on mortality data from 2023. Once again, heart disease reigned supreme as the leading cause of death in the United States1 – a sorry distinction it has held firmly for the last two decades.
Heart disease – and more specifically, coronary atherosclerosis, which is responsible for the majority of deaths from cardiovascular disease – is easily the most preventable of all the “four horsemen of chronic disease” (i.e., heart disease, cancer, neurodegenerative disease, and metabolic disease). It is causedby apoB-containing lipoproteins (90-95% of which are low-density lipoproteins, or LDLs), which penetrate artery walls and initiate atherogenesis. Thus, therapies for lowering circulating LDL levels – such as statins, PCSK9 inhibitors, and others – have the power to virtually stop atherosclerosis in its tracks. So why does this disease remain a top killer? A study published last month provides some insights, along with further evidence of the importance of lowering LDL as a means of preventing atherosclerosis-related mortality.2
About the study
Study authors Faridi et al. analyzed data from the Miami Heart Study, which involved participants who were 40-65 years of age and free of any clinically evident cardiovascular disease (CVD) at enrollment.3 From this cohort, the present study excluded any participants with additional risk factors for atherosclerosis, including hypertension (systolic blood pressure ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg), diabetes, or tobacco use, as well as any individuals who were taking lipid-lowering medications. This left Faridi et al. with a final cohort of 1,033 participants (median age of 51 years at the time of enrollment; 55% women) with no CVD symptoms and at relatively low risk based on the exclusion criteria.
As part of the original Miami Heart Study, participants had undergone cardiac imaging tests at baseline, including coronary artery calcification (CAC) scans and contrast-enhanced coronary computed tomography angiography (CCTA) scans. Laboratory tests were also performed to assess baseline blood lipids. In the present study, Faridi et al. utilized these cross-sectional baseline data to determine the prevalence of coronary atherosclerosis among low-risk, asymptomatic adults, as well as to characterize its associations with atherogenic lipoprotein concentrations as estimated by LDL cholesterol (LDL-C) or non-HDL-cholesterol (non-HDL-C), or directly measured by apoB levels.
A high prevalence of atherosclerosis in low-risk adults
Despite their evident “low risk” status, over one third (35.9%) of participants included in the analysis were found to have coronary plaque, while roughly one quarter (25.3%) had a CAC score over zero – an indication of the presence of early-stage artery calcification. Additionally, a smaller set of participants were found to have more advanced CVD, with 4.5% having CAC scores ≥100 (indicating moderate disease), 3.4% showing evidence of high-risk plaque, and 1.9% demonstrating artery blockage of at least 50% according to CCTA scans.
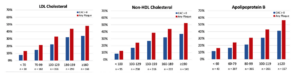
The proportion of participants with coronary plaque increased with increasing serum levels of LDL-C, non-HDL-C, and apoB (see Figure below). Specifically, after adjusting for covariates, each 10 mg/dL increase in LDL-C was associated with a 13% increase in risk (OR: 1.13; 95% CI: 1.08-1.18), each 10 mg/dL increase in non-HDL-C was associated with a 12% increase in risk (OR: 1.12; 95% CI: 1.08-1.16), and each 10 mg/dL increase in apoB was associated with a 20% increase in risk (OR: 1.20; 95% CI: 1.13-1.27). The somewhat stronger association between plaque and apoB compared to associations with LDL-C or non-HDL-C is in line with expectations, as atherogenesis depends on the number of apoB-containing lipoproteins (as indicated by apoB levels) rather than on their cholesterol content (as indicated by LDL-C or non-HDL-C). Importantly, the increases in risk with increasing lipoprotein levels appeared to be linear down to at least 70 mg/dL LDL-C – well below the American Heart Association’s current guideline of <100 mg/dL as an “optimal” value.4 Across lipoprotein strata, risk was also observed to increase with age and was higher among men than among women, which agrees with earlier reports on sex differences in atherosclerosis progression and adverse cardiovascular events.5
Figure: Prevalence of coronary atherosclerosis among low-risk adults based on serum lipid and lipoprotein concentrations. Prevalence of coronary atherosclerosis (as detected by CCTA) and coronary artery calcium (as detected by CAC scan) is shown as a percentage of participants within each stratum of lipoprotein levels. Cholesterol values are in mg/dL. Adapted from Faridi et al. 2024.²
The authors also performed analyses on a subgroup consisting of the very lowest-risk participants, defined by more stringent risk factor thresholds than the full cohort (e.g., systolic blood pressure <120 mm Hg, diastolic blood pressure <80 mm Hg, BMI <25 kg/m2). Within this subgroup (n=184; 83.7% women), prevalence of coronary plaque was lower than in the full cohort but still alarmingly common, as it was observed in 21.2% of these “optimal risk” participants. CAC scores above zero were reported for 14.7% of the subgroup, though none of these participants demonstrated CAC scores ≥100 or ≥50% artery blockage.
A silent but avoidable killer
In all, Faridi et al.’s results reveal a startlingly high prevalence of early- to moderate-stage coronary atherosclerosis among patients classified as “low risk” with no reported symptoms such as chest pain or shortness of breath. Further, they show that higher levels of apoB-containing lipoproteins were associated with higher risk, even when comparing levels below those regarded as optimal by current guidelines. While this was an observational study based on cross-sectional data and on its own tells us nothing about any causal relationship between apoB and cardiovascular disease, these results align with a large, consistent body of evidence indicating that apoB-containing lipoproteins drive the development of atherosclerosis – and that reducing serum levels of apoB-containing lipoproteins, for instance with statins or PCSK9 inhibitors, can slow or halt the progression of this disease and help to prevent subsequent major adverse cardiovascular events such as heart attacks or strokes.
Thus, we return to the question posed at the start of this piece – why is atherosclerotic cardiovascular disease so deadly despite the existence of effective treatments? The results of the present study suggest a simple (albeit alarming) answer: millions of individuals with this disease are likely unaware of it. Atherosclerosis develops over decades of exposure to high levels of circulating apoB-containing lipoproteins, yet for those who are relatively young or otherwise healthy, both patients and physicians often ignore the possibility of coronary artery disease, failing to test for it via CAC or CCTA scans even when LDL-C is known to be elevated.
Faridi et al.’s data show that apparent health is no guarantee of the absence of CVD, and as we’ve seen in a previous newsletter, being proactive about lipid and imaging tests – and following up with appropriate treatments – can literally be the difference between life and death. On a population scale, these actions have the power to put an end to mortality from coronary atherosclerosis. One horseman down, three to go.
The pharmacies are already advertising: Get your flu shot now.
Is this really the best time to get your flu shot when influenza rates are low, and the vaccine has a tendency to wear off?
The timing game
There is no one-size-fits-all answer. Personally, my plan is to wait until mid-October to get my annual flu shot. I’ll be keeping an eye on estimated flu rates in the U.S. and might move that target date forward or even a little back depending on how things are going.
I’m getting my updated Covid shot as soon as I can though, hopefully in early September if not sick before then.
The timing of the annual flu season — as determined by elevated flu activity – varies from season to season. During most seasons, activity begins to increase in October, most often peaks between December and February, and can remain elevated into May.
It’s rare, but not impossible, to have influenza peaks in the early fall. Over the past 20 years, here is when the peaks have occurred, with February taking the gold medal:
Other medical experts generally recommend getting the annual flu shot in early fall, typically by the end of October. This timing is based on several factors:
Waning protection: The flu vaccine’s effectiveness can decrease over time, with studies suggesting a gradual decline in protection over 6 months.
Peak flu season: In the Northern Hemisphere, flu activity typically peaks between December and February, although it can last as late as May.
Immune response time: It takes about two weeks after vaccination for antibodies to develop and provide protection against the flu.
Unique personal risks: Older adults (65+) and those with weakened immune systems might benefit from slightly later vaccination (e.g., in October) to ensure protection keeps up through the entire flu season.
Besides the flu shots, there are a lot of other shots vying to get in our arms, too. According to CDC and UpToDate, it is OK to give the flu shot with and updated Covid shot, or an RSV shot, or a pneumonia shot. However, if we are diligent and reliable with follow through, I like to spread mine out, with a couple weeks in between flu and Covid shots… especially this year since we are enduring a massive Covid wave right now. The sooner we can get updated JN.1 or KP.2 shots in the arms of people who have not had Covid during this wave the better.
Unlike Covid, U.S. flu activity is estimated to be very low right now. You can check in on this by following the weekly CDC influenza activity map. Of course, they use a wide array of red/green colors for the 1 out of 12 men who are red/green colorblind. No respect:
Overall efficacy
Depending on the year and how well matched the vaccine is, protection against infection ranges from 50 to 80%. But pooling all those years together we get the following averages:
Vaccination is associated with a reduced incidence of contracting influenza:
In a 2018 meta-analysis including eight trials and more than 5000 adults ≥65 years, influenza vaccination reduced the incidence of influenza from 6 to 2.4 percent, for about a 58% reduction in cases [45].
Among vaccinated individuals with breakthrough influenza virus infection, vaccination is associated with reduced mortality and attenuated disease severity [46]:
Among five observational studies of adults with influenza-associated hospitalization, vaccination was associated with 31 percent mortality reduction.
Among eight studies of adults with influenza-associated hospitalization, vaccination was associated with 26 percent reduction in odds of intensive care unit admission.
How long does the flu shot provide protection?
Some protection is durable, but the highest protection is in the first month or two.
Flu vaccine effectiveness wanes 9% every 28 days, starting 41 days post-vaccination in adults (but not in children, who were found to have stable protection throughout the whole season!), according to a study published this year in Eurosurveillance. The study went out to 5 months after flu vaccination and found that overall:
Our results were comparable with other studies examining protection by time since influenza vaccination. A study from Singapore (which has year-round influenza activity due to its tropical climate) found that the infection odds increased 1.07 times every 8 weeks since vaccination [8]. A study in the US found that the odds of influenza A(H3N2) infection increased 1.12 times every 14 days [16]. Another US study found that the odds of influenza increased 1.16 times every 28 days [9].
What’s in the flu shot this year?
Are they still quadrivalent (covering 4 strains)?
For the 2024-25 season, all influenza vaccines available for administration in the United States will be trivalent (covering three types), containing a representative strain of influenza A/H1N1, influenza A/H3N2, and influenza B/Victoria lineage.
Viruses of the influenza B/Yamagata lineage have not been identified globally since March 2020, and the WHO and other public health authorities have recommended that it be removed from the seasonal vaccine.
Every case of flu prevented matters. Just like Covid, flu can do bad stuff under the hood. Did you know that undiagnosed influenza occurs in almost 10% of people admitted with heart attacks, especially during the flu season? I’m going to highlight a recent NEJM study about this in a future quick post, but here is the bottom line:
Results showed that the overall risk of heart attack was 6.16 times higherin the week after influenza infection. Notably, this risk was significantly higher (16.60 times!) for individuals without prior coronary artery disease.
So, does getting a flu shot reduce the above risk of cardiovascular complications? Yes. In a study published in 2020 looking at high risk people(defined as people over age 50 (yikes, that’s almost me!), HIV/AIDS patients, those residing in nursing homes, and people who are obese), getting a flu shot was associated with a:
28% reduced risk of heart attack
47% reduced risk of TIA
73% reduced risk of death.
I’ll stop there as I think you get the point, despite many people trivializing flu shots. But more “patient education” can be read here via UpToDate if you want more.
The experts say that good flu shot bets are usually placed in October, but keep your eyes on this year’s actual flu trends. Spread the word and forward at will. And as they say, talk to your doctor 😉
Labels for GLP-1 medications, like Ozempic and Mounjaro, might see more approved uses as researchers study the drugs’ effects on sleep apnea, dementia and other health issues. Meanwhile, oncologists are looking at a GLP-1 role in cancer care.
Several studies have shown the therapies — currently approved for Type 2 diabetes and weight loss — can diminish the risk of multiple cancers:
Delaware finally amended its DMV reporting laws to no longer require mandatory reporting of patients with seizures, loss of consciousness or other medical conditions.
Physicians should continue to use their medical judgment when dealing with patients with potentially impaired driving capabilities and may continue to send reports to DMV on a case by case basis.
House Bill 314, which updates the outdated mandatory reporting requirements for loss of consciousness due to a central nervous system condition, was supported by MSD and had passed both chambers. On Friday, August 2nd, Governor Carney signed the legislation into law.
MSD President, Robert Varipapa, MD, testified that the mandatory reporting system did not function effectively, especially in the emergency room setting where individuals are often inappropriately reported to the Division of Motor Vehicles (DMV) resulting in overworked DMV personnel and a substantial backlog in the physician’s office.
It was also noted that the mandatory reporting requirement placed physicians in the awkward role of being a law enforcement officer, leading some patients being hesitant to truthfully disclose seizures or other episodes of loss of consciousness to their physician due to fear of losing their license.
MSD testimony stated that physicians and other medical professionals should still report cases to the DMV based on medical evidence, not only limited to repeated loss of consciousness, but also other conditions such as dementia and stroke.
This Act does all of the following:
(1) Allows for all licensed practitioners (physician, nurse practitioner, or physician assistant) who are treating a driver for a medical condition to report findings and sign Division paperwork, which mirrors verbiage found in Title 24;
(2) Updates the name of Medical Council to Board of Medical Licensure and Discipline which ensures compliance with code in handling of individual cases; and
(3) Changes the Secretary of Health and Social Services to Secretary of Transportation for determining the status of driver’s license for individuals with a potential medical condition which allows for quicker response and ensures the confidentiality of a driver. Lastly it removes a section from the Medical Licensure Act consistent with the other provisions of the bill.
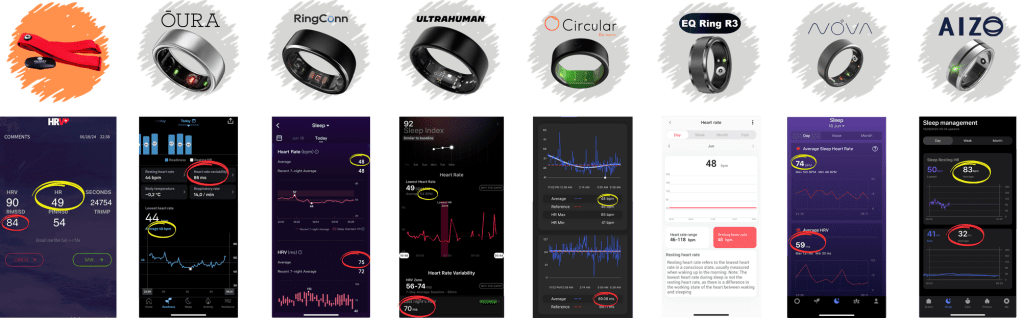
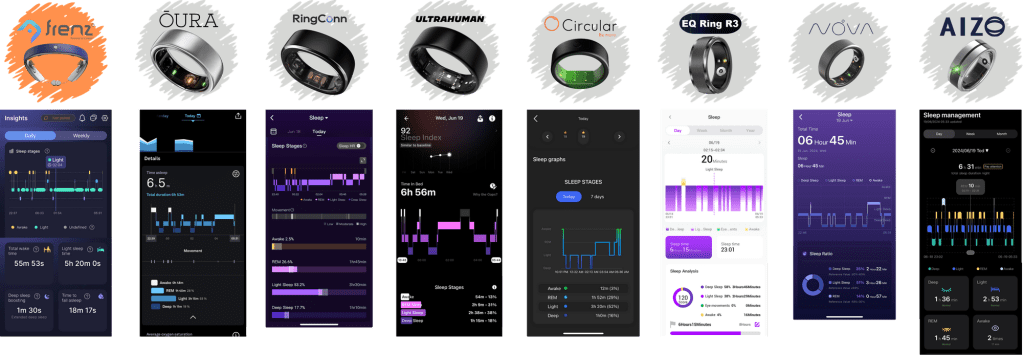
‘Wearables’ are a great way to monitor a variety of health parameters, including general activity, workouts, heart rate, heart rate variability, sleep, among others.
If you’re not into an Apple Watch or Fitbit, you might want to try a wearable ring, seven of which are compared in the linked article in much detail.
Oura is probably the most known of the seven rings but I would suggest also looking at Ultrahuman (no subscription) and RingConn (lots of charts and longest battery life.)
PS: RingConn is releasing a ‘Gen2’ ring on Kickstarter for around $200, which is a great deal. Their ring has great battery life, is the smallest of all the rings, doesn’t require a subscription and features sleep apnea monitoring.
Offit and other experts said there are two possible reasons that the shingles vaccine might protect against dementia. First, previous research suggests that herpes infection might play a role in the development of dementia.
Shingrix dramatically decreases the reactivation of the herpes virus that causes chickenpox. It’s 97 percent effective at preventing shingles in people ages 50 to 69 with healthy immune systems, according to the CDC.
Experts also hypothesize there might be something about the particular way Shingrix stimulates the body’s immune system against shingles that decreases the chances of dementia.”